Welcome to DU!
The truly grassroots left-of-center political community where regular people, not algorithms, drive the discussions and set the standards.
Join the community:
Create a free account
Support DU (and get rid of ads!):
Become a Star Member
Latest Breaking News
General Discussion
The DU Lounge
All Forums
Issue Forums
Culture Forums
Alliance Forums
Region Forums
Support Forums
Help & Search
Rethinking the homunculus

When we discovered that the brain contained a map of the body it revolutionised neuroscience. But it’s time for an update
https://aeon.co/essays/the-iconic-brain-map-thats-changing-neurosurgery-and-gaming

Dagmar Turner, a violinist, during surgery to remove her brain tumour, January 2020. Photo courtesy King’s College Hospital, London
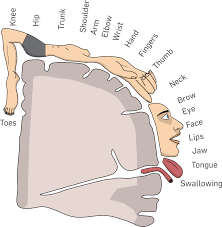
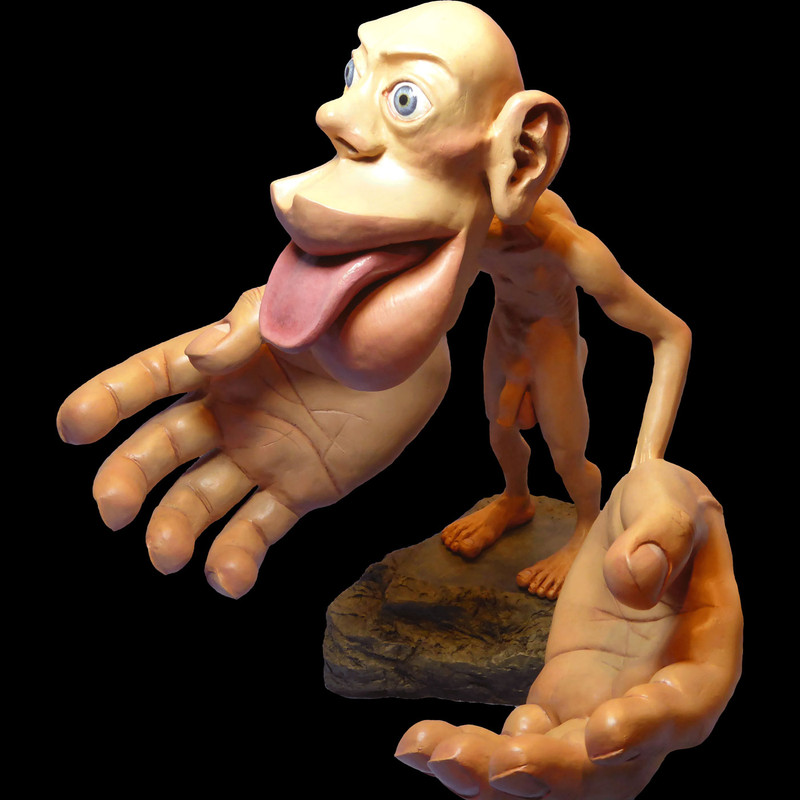
The homunculus is one of the most iconic images in neurology and neuroscience. Usually visualised as a series of disproportionately sized body parts splayed across a section of the brain, it shows how the body is systematically mapped onto the sensory and motor cortices, representing the proportion of brain tissue devoted to each part of the body. This image has not only had a long-lasting impact on neurosurgical practice and basic brain research, but has also entered the public imagination, with three-dimensional clay models consisting of an enormous head and outsized hands attached to a tiny torso, on display at the Natural History Museum in London, and elsewhere. The groundbreaking work that led to the homunculus was a major advance in our understanding of the structure and function of the brain, and the homunculus itself revolutionised the art of medical illustration. Yet modern research suggests that the homunculus is far more complex than originally thought, and some argue that it is incorrect and needs to be radically revised.
The homunculus – meaning little man – is the brainchild of the Canadian neurosurgeon Wilder Penfield (1891-1976), who co-founded the Montreal Neurological Institute at McGill University in 1934 and became its first director. There, he developed a pioneering technique for identifying, and then surgically removing, abnormal brain tissue causing epileptic seizures. Using this method over the course of his career, he and his colleagues produced early detailed maps of the functions of various regions of the cerebral cortex. Most epileptic patients respond well to anti-convulsant drugs, but for those who do not, and whose seizures become frequent, severe and debilitating, brain surgery is a last-resort treatment. Penfield’s technique involved using an electrode to electrically stimulate the surface of the patient’s brain; crucially, they remained fully conscious on the operating table during the procedure, so that the patient could describe the effects of the stimulation. This enabled Penfield to cut out, or resect, the tissue causing the seizures without damaging neighbouring tissue involved in functions such as movement and language.
With the patient’s scalp anaesthetised and their skull opened, Penfield applied small electrical currents to the exposed surface of his patient’s brain. Because the patient remained fully conscious, Penfield could not only observe the movements evoked by stimulation of a specific area, but also ask them about the sensations and perceptions they experienced. Penfield operated on more than 1,000 patients throughout the 1930s and ’40s, and thus comprehensively ‘mapped’ the function of each area of the cerebral cortex. Electrical stimulation of some regions elicited the recall of long-lost memories; others triggered musical or olfactory hallucinations, famously causing one patient to report: ‘I smell burnt toast!’ His most important discovery, however, was the organisation of the sensory and motor cortices, two narrow, adjacent strips of tissue that run down from the top to the bottom of the brain on either side of the central sulcus, a deep fissure separating the frontal and parietal lobes.

Here, stimulation in front of the fissure evoked small movements or muscle twitches in specific parts of the body, and stimulation just behind it evoked sensations instead. Importantly, the body appeared to be mapped in a highly organised manner in both of these regions, such that stimulation of adjacent patches in either evoked movements or sensations in adjacent body parts on the opposite side of the body. Thus, stimulation of the top of the brain evoked movement or sensation in the hip and torso, and stimulation progressively further down along the outer surface elicited responses first in the shoulder, arm, elbow, forearm, and then the wrist. Finally, there was a large patch of both strips of tissue devoted to the hand, with each finger represented individually, and another large patch devoted to the face, tongue and throat. Crucially, although the precise size and location of the tissue devoted to each body part differed between patients, the sequence of responses elicited by progressive stimulations from the top to the bottom of the brain was always the same. During each procedure, Penfield would place small numbered stickers on the patient’s brain, and take note of the response evoked by electrical stimulation of that particular patch of tissue (see figure below):
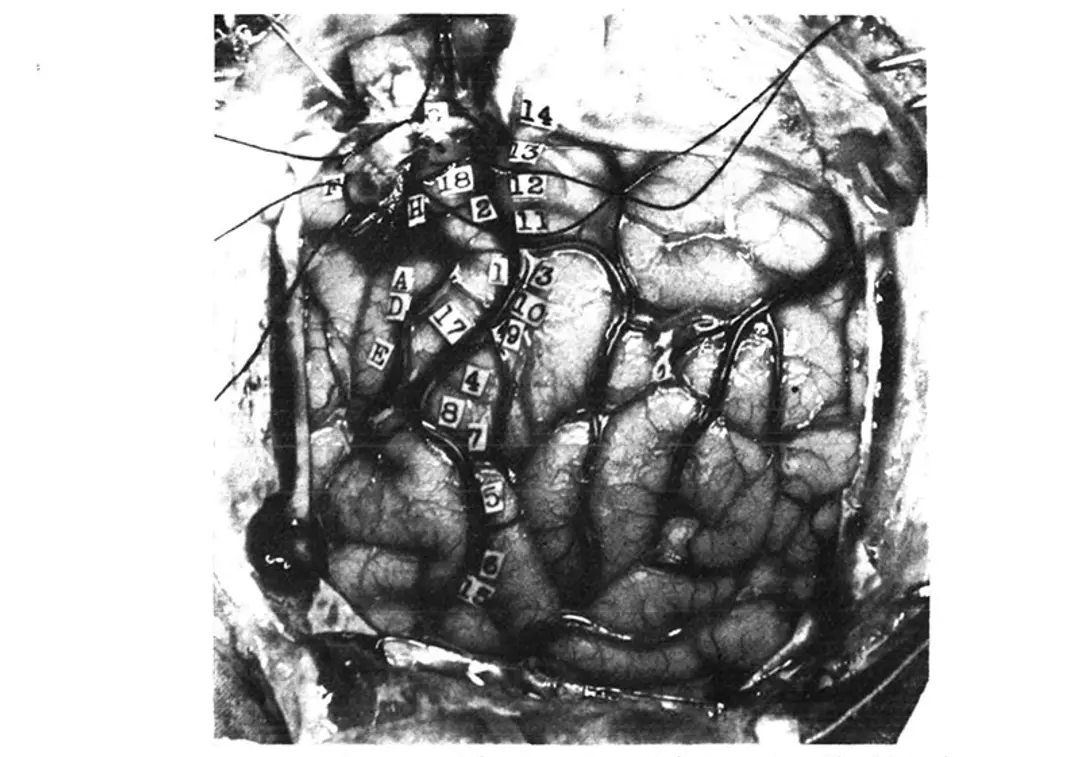
From Wilder Penfield and Edwin Boldrey’s 1937 paper. American Neurological Association
14. Tingling from the knee down to the right foot, no numbness.
13. Numbness all down the right leg, did not include the foot.
12. Numbness over the wrist, lower border, right side.
11. Numbness in the right shoulder.
3. Numb feeling in hand and forearm up to just above the forearm.
10. Tingling feeling in the fifth or little finger.
9. Tingling in first three fingers.
4. Felt like a shock and numbness in all four fingers but not in the thumb.
8. Felt sensation of movement in the thumb; no evidence of movement could be seen.
7. Same as 8.
5. Numbness in the right side of the tongue.
6. Tingling feeling in the right side of the tongue, more at the tip.
15. Tingling in the tongue, associated with up and down vibratory movements.
16. Numbness, back of tongue, mid-line.
Precentral gyrus from above down: –
(G) Flexion of knee.
18. Slight twitching of arm and hand like a shock, and felt as if he wanted to move them.
2. Shrugged shoulders upwards; did not feel like an attack.
(H) Clonic movement of right arm, shoulders, forearm, no movement in trunk.
(A) Extreme flexion of wrist, elbow and hand.
(D) Closure of hand and flexion of his wrist, like an attack.
17. Felt as if he were going to have an attack, flexion of arms and forearms, extension of wrist.
(E) Slight closure of hand; stimulation followed by local flushing of brain; this was repeated with the strength at 24. Flushing was followed by pallor for a few seconds.
(B) Patient states that he could not help closing his right eye but he actually closed both.
(C) Made a little noise; vocalisation. This was repeated twice. Patient says he could not help it. It was associated with movement of the upper and lower lips, equal on the two sides …
snip
InfoView thread info, including edit history
TrashPut this thread in your Trash Can (My DU » Trash Can)
BookmarkAdd this thread to your Bookmarks (My DU » Bookmarks)
2 replies, 731 views
ShareGet links to this post and/or share on social media
AlertAlert this post for a rule violation
PowersThere are no powers you can use on this post
EditCannot edit other people's posts
ReplyReply to this post
EditCannot edit other people's posts
Rec (7)
ReplyReply to this post
2 replies
 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
Rethinking the homunculus (Original Post)
Celerity
Mar 1
OP

dweller
(23,641 posts)1. Homunculus brain and body
Male
Female

✌🏻

Delphinus
(11,831 posts)2. This is
simply fascinating!